Dr. Jacques Duff Psychologist, Clinical Neuroscientist and Nutritionist
There has been increasing professional and public concern about the increase in the incidence of Autism Spectrum Disorders (ASD) and Attention Deficit/Hyperactivity Disorder (ADHD) over the last decades.
Recent research suggests that these disorders are associated with genetic predispositions triggered by environmental factors [1-6]. Factors such as a “Western style” diet, consisting of too many nutrient-poor refined foods, additives, preservatives and colourings [7], and other chemicals. In 2008 the European Union mandated to put warnings on foods containing some of these harmful additives:
“THIS FOOD MAY HAVE AN ADVERSE EFFECT ON ACTIVITY AND ATTENTION IN CHILDREN”.
However, despite mounting evidence, the US and Australia have not taken such action. Other factors, such as pre-natal and peri-natal maternal stress [8] and environmental toxins [9] have also been associated with a greater risk for Autism.
Duff (2013) outlined the scientific basis as to why environmental and nutritional factors may be to blame for this rising problem [10]. Children and adolescents with poor nutritional status suffer from alterations of mental function and behavioural problems that can be corrected by dietary measures [11]. A University of Sydney study has found that adolescent boys being treated for ADHD with stimulant medications have a dose dependant reduction in growth during puberty [12]. Hence, since these disorders are triggered by lifestyle, nutritional and environmental factors, these are the factors that require the most attention in research and treatment, followed by which behavioural treatment method is most effective.
The child with mild ADHD or Autism generally struggles at school and in adulthood but is capable of achieving academically and in life, albeit with much effort and after much parental stress and social problems. However, for those with more severe symptoms, the future may be bleak. Research shows that as adults, those with more severe ADHD tend to fail to achieve academically, change employment more often and have more failed relationships and University drop outs. Many with co-morbid Oppositional Defiant Disorder can develop conduct disorder as teens, leading to antisocial personality disorder or criminality in adulthood [13]. The child with severe Autism is usually dependant on care givers for life [14]. Many families split on account of the stress, leaving single mothers to care for their disabled dependent child.
The Autism (ASD) problem:
The number of children diagnosed with ASD has and is still growing at an alarming exponential rate.
- In the 1950s it was estimated that 1 in 25,000 children was diagnosed with Autism.
- In 1970s and 1980s, about one in 2,500 children was diagnosed with ASD.
- In 2000, the US Centre for Disease Control (CDC) reported that the prevalence of ASD had reached 1 in 150 children.
- In 2004 this figure had reached 1 in 125 children
- In 2006 The figure was one in 110 children
- In 2008 this figure reached 1 in 88, based on the CDC’s ADDM network of 14 monitoring areas across the US. These ranged from 1 in 208 in under-populated states to one in 47 in populated eastern states.
- In March 2013, the US National Health Statistics Report indicated that 1 in 50 children across the US were diagnosed with ASD. In populated US cities this is already 1 in 27 children.
If one extrapolates the trend from these figures as shown in the following graph, we could easily be looking at a 5% incidence in Autism by 2020. That is one child in every 20 children across the US having a diagnosis of ASD by 2020.
Actual and projected % Prevalence of Autism in the US
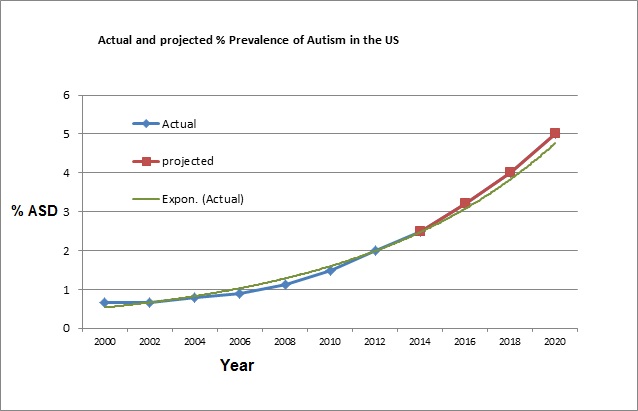
In the above graph, statistics from CDC (2000 to 2008) and the US National Health Statistics Report (2013), Projection to 2020, indicate that the incidence of Autism is rising exponentially.
The worse is yet to come, as there is no plan and very little prevention and research in dietary and environmental factors being done to kerb the growth in autism.
Prevalence of Autism (ASD) In Australia.
According to the Australian Bureau of Statistics Survey of Disability, Aging and Carers (SDAC) figures:
- In 2003, 30,400 Australians had autism.
- In 2009, 64,600 Australians had autism.
- In 2012, 115,400 Australians had autism.
In 2012, the incidence of Autism in children between the ages of 5 and 9 in Australia was 1 in 32 children.
Causes of Autism (ASD)
The exact causes of Autism in general, and for each individual child with Autism remain elusive. Scientists have been researching the “gene” that may cause Autism, amongst families with Autism, with no success. This is not surprising, as single genes that cause a specific disease (as in cystic fibrosis) are very rare. However, there is widespread agreement amongst scientists involved in Autism research that Autism arises from a combination of a cluster of mutated genes (the genetic predispositions), interacting with nutrient deficiencies in our modern diet and environmental toxins. This view is consistent with epigenetics research, which teaches us that factors outside of genes profoundly affect their expression.
ASD Genetic predispositions
Humans have around 25,000 genes which make around 100,000 proteins or enzymes that carry out a multitude of functions in the body. Autism is associated with a combination of a dozen or so common polymorphisms (mutations) that seem to be over-represented in the ASD population. Many of the same mutations are also over-represented in other modern diseases, such as cancer. These genes are involved in the following functions:
- Some produce enzymes that are involved in converting dietary vitamins such as Folate, Vit. B12 and Vit. B6 to their active form.
- Others are involved in detoxing in the liver to remove toxins from blood circulation.
- Others work inside the cells to neutralise toxins and oxidative free radicals.
- Others regulate a myriad of biochemical reactions that keep us healthy.
These enzymes require proteins, vitamins and minerals as co-factors for their synthesis and functions. Hence, genetic mutations combine with the lack of nutrient co-factors and toxic overload to precipitate malfunctions in key enzymes. This is the process that is believed to underpin the increase in modern diseases in adults, as well as Asthma, Eczema, Autism, ADHD, Learning Difficulties and other Neurodevelopmental disorders in our young.
Nutrient deficiencies
We evolved as a species over millions of years on account of interactions between our genes, our immune system, our diet and the environment. This process of adaptation has optimised the body of our evolutionary ancestors. Whenever we ingest something, it is tested at a molecular level by out immune cells to determine if it is friend or foe (antigen). Antigens are attacked our immune system, resulting in inflammation or even autoimmune disorders. Our modern “Western style” diet is a far cry from that of our ancestors in the Paleolithic period. The diet that we evolved on was nutrient dense and derived from virgin volcanic soils, rich in minerals, whilst our soil in Australia and the US lacks the minerals found in volcanic soils. To increase yield and pest resistance, we use genetic selection and irridiation, pesticides, and chemical fertilisers that produce nice looking but nutrient-poor crops. Furthermore food processing destroys around 70% of the vitamins and micronutrients in much of our day to day processed staple foods, such as breakfast cereals, bread and pasta.
The Toxicity of Wheat
Epidemological studies indicate that the increased prevalence of modern diseases, ASD and ADHD is associated with a western style diet (such as nutrient-poor processed foods, food additives, colourings and preservatives) and environment factors such as lifestyle and pollution.
Our Modern wheat has a short stem, the result of the introduction of dwarfing genes in the 1960s by Norman Borlaug. He won the Nobel Peace Prize in 1970 for his work in back crossing hybrid species of wheat for robustness, increase yield and pest resistance. This genetically engineered new wheat species contains extremely high levels of Wheat Germ Agglutinin (WGA), a Lectin that protects wheat from insects, yeast and bacteria by disrupting structures containing N-acetyl-D-glucosamine and Sialic acid in their bodies and killing these pests. At such high concentrations, WGA has the potential to bind to and disrupt the integrity and function of the following tissues and promoting inflammation:
- Joint cartilage.
- Mucous membranes, e.g. the lining of the inner nose and lungs
- Mucous lining of the digestive tract and intestines.
- Arteries around the heart.
- Beta pancreatic cells that are involved in making Insulin.
- Hippocampal brain cells
- The cornea of the eye.
There are also health issues with other aspects of gluten. If there is an overgrowth of Streptococcus bacteria in the bowel (caused by too much grains, animal proteins and refined carbohydrates and not enough fruit and vegetables). The Strep produces an enzyme Streptococcal Kinase which binds to the DPP-IV digestive enzymes needed to breakdown gluten and casein. This resulting lack of DPP-IV results in gluteomorphine and casomorphine being produced due to inadequate denaturing of gluten and caseine. These exorphins can have a myriad of opiate-like effects on the brain resulting in a dulling of cognitive skills.
Many people have the genes for Coeliac disease without overtly having Coeliac disease. However, these carriers are much more likely to have Irritable Bowel Syndrome for years before eventually developing Coeliac disease which results in damage to the intestinal villi. A Coeliac Serology is only positive when the IBS condition has deteriorated to the point of damaged villi and elevated titres.
The need to address root causes of ASD and ADHD
Unless we address the root causes and educate the public and policy makers, Pharmaceutical companies will continue to seek medical solutions to treat these disorders and will continue to convince our doctors and policy makers that “medication” is best practice.
Unless we bite the bullet and publish more research that shows that we can reverse these trends through changes in diet, nutrition, and lifestyle factors, thirty years from now, we will have a greatly reduced able-adult population. Our children and grand children will live in a world where the health and economic costs of an increasingly ageing and disabled population will be unsupportable.
Prevention better than cure.
The old adage “An ounce of prevention is better than a pound of cure” has never been so relevant. Most of the research nowadays is directed towards funding medical treatments and hopefully cures. However, the reality is that for Autism and ADHD, there have been no medical advancements in disease prevention, and there are with no medical cures in sight.
For Cancer and Cardio Vascular Disease, there have been many advances in early detection, and better treatment outcomes, which mean that survival rates are higher. However, very little research is being done in prevention. Hence, the incidence is rising faster than ever.
There are no medications that address the symptoms for Autism.
Early Intensive Behavioural Intervention (ABA therapy)
The Government-recommends and funds Early Intensive Behavioural Intervention. This involves a minimum 40 hours per week of treatment with either a Behavioural Psychologist, Behavioural Therapist, Speech Pathologist, and Occupational Therapist. We still use the same ABA based intensive early intervention treatment methods, developed in the 70s for Autism, with minor methodological improvements. Government funding (FaCHSIA) provides a maximum of $12,000 to be spent over 2 financial years before turning 7, and Medicare funding of a maximum of 10 sessions a year.
If all of the required therapy was to be provided by suitably trained Health professionals (FaCHSIA approved providers) the cost can conservatively be between $2000 to $6,000 a week. Many families with disposable income currently spend around $100,000 a year to fund treatment. However, most families compromise and engage unqualified therapists who are often improperly supervised. The pressures are such that many families split, and single mothers are left to shoulder an unbearable burden. Some families mortgage or sell their homes to fund treatment. All too often, families do a minimum of inadequate treatment (4-6 hours a week), often provided by ill-trained and unsupervised therapists because they are cheaper. Some families are so overwhelmed that they do nothing, and the child receives no treatment at all, and grows up to be a disabled adult and a burden to his family and the community.
Pivotal Response Treatment
We advocate the use of Pivotal Response Treatment (PRT), an Early Intensive Behavioural Intervention technique developed at the University of California in Santa Barbara at the Koegel Autism Centre. This is a treatment model which trains and encourages parents and caregivers to provide the treatment themselves in the child’s own environment. In this model an Autism-expert Psychologist designs and supervises a treatment program implemented by parents, caregivers and therapists as needed. It is the best researched and most effective behavioural intervention to-date.
PRT can reduce the cost of treatment to $300 - $1000 a month. Provided that the parents are able to do much of the therapy themselves, under guidance of an expert Psychologist, who designs and monitors the program. This model is not suitable for all families for a variety of reasons. The model is inappropriate for example: when both parents have to work, when there is a single parent family, when other children demand the parents’ time, or when there is more than one child with autism in the family.
Bowel and Gut Dysfunction in Autism (ASD)
Children with ASD, more often than not, have very disrupted intestinal function, characterised by diarrhoea or constipation or alternating between both conditions. They also tend to have a very limited and self-restricted diet, severely lacking in nutrients. We recommend blood tests to investigate nutrient deficiencies. This is a practice frowned upon by mainstream Medicine and Medicare, despite many published studies supporting this approach.
Research indicates that there are genetic polymorphisms that are over-represented in autism, and these affect cellular detoxing, leading to cellular malfunction from poor diet, and environmental toxins. After suitable investigations, we recommend dietary changes and nutritional supplementation to redress deficits, and we train parents in the implementation of suitable diets. Our ASD children improve more rapidly when diet, nutrient and environmental factors are addressed in conjunction with PRT.
However, most health professionals have not been trained in Neuroscience or Nutritional and Environmental Medicine, they still follow the general consensus, from decades ago that Autism is largely untreatable. Intensive education of policy makers, parents and health professionals is badly needed.
The ADHD problem:
Almost every child with Autism has Attention deficit-hyperactivity disorder (ADHD). ADHD is a neurobehavioral disorder which is characterized by significant difficulties of inattention or hyperactivity and impulsiveness or a combination of both. According to the current Diagnostic and Statistical Manual of Mental Disorders (DSM-V), symptoms emerge before seven years of age.
Recent US surveys asked parents whether their child received an ADHD diagnosis from a health care provider. The results show that:
- Approximately 11% of children 4-17 years of age have been diagnosed with ADHD as of 2011.
- The percentage of children with an ADHD diagnosis continues to increase, from 7.8% in 2003 to 9.5% in 2007 and to 11.0% in 2011.
- Rates of ADHD diagnosis increased an average of 3% per year from 1997 to 2006 and an average of approximately 5% per year from 2003 to 2011.
- Boys (13.2%) were more likely than girls (5.6%) to have ever been diagnosed with ADHD.
- The average age of ADHD diagnosis was 7 years of age, but children reported by their parents as having more severe ADHD were diagnosed earlier.
source http://www.cdc.gov/ncbddd/adhd/data.html
Research and clinical evidence suggests that ADHD management should start with lifestyle and dietary changes and individual supplementation of appropriate nutrients. Depending on the results of QEEg (Brainmapping) analysis some children should undergo Neurotherapy treatment to suppress excessive slow brainwave electrical activity. Some children may need to be medicated in the short to medium term to allow them to function adequately while the dietary, nutritional and Neurotherapy has time to work.
The psychostimulant medications for ADHD (Ritalin and Dexamphetamine) are exactly the same stimulant drugs that were introduced over 50 years ago. Despite the billions spent each year, cures are nowhere in sight. The drugs for ADHD are only useful for around half of the children with ADHD and for some have undesirable, often unacceptable side-effects.
Neurotherapy has been shown, in dozens of published papers, to be as effective as psychostimulant drugs in the treatment of ADHD and without any of the drug side-effects. A number of recent scientific papers have recommended Neurotherapy as primary treatment for ADHD. Yet acceptance in medical circles is very poor.
Our proposed solution
- More Public awareness and education and Government advocacy regarding the scientific evidence available to support a prevention and treatment model that incorporates nutritional and environmental factors and Neurotherapy.
- A "World class' treatment and research centre, where treatment based on all available scientific evidence, is conducted, guided by an expert Scientific Advisory Committee.
- Treatment outcomes will be documented and outcome-research papers published in scientific journals.
- The foundation will provide subsidised treatment to needy families (through philanthropic, government and business support)
- Such a centre will be a guiding light to other health professionals and the public throughout Australia.
References
- Kawicka, A. and B. Regulska-Ilow, How nutritional status, diet and dietary supplements can affect autism. A review. Rocz Panstw Zakl Hig, 2013. 64(1): p. 1-12.
- Dauncey, M.J., Genomic and epigenomic insights into nutrition and brain disorders. Nutrients, 2013. 5(3): p. 887-914.
- Essa, M.M., et al., Excitotoxicity in the pathogenesis of autism. Neurotox Res, 2013. 23(4): p. 393-400.
- Brown, A.C. and L. Mehl-Madrona, Autoimmune and gastrointestinal dysfunctions: does a subset of children with autism reveal a broader connection? Expert Rev Gastroenterol Hepatol, 2011. 5(4): p. 465-77.
- Engel, S.M. and J.L. Daniels, On the complex relationship between genes and environment in the etiology of autism. Epidemiology, 2011. 22(4): p. 486-8.
- Bell, S.J., G.T. Grochoski, and A.J. Clarke, Health implications of milk containing beta-casein with the A2 genetic variant. Crit Rev Food Sci Nutr, 2006. 46(1): p. 93-100.
- Millichap, J.G. and M.M. Yee, The diet factor in attention-deficit/hyperactivity disorder. Pediatrics, 2012. 129(2): p. 330-7.
- House, S.H., Nurturing the brain nutritionally and emotionally from before conception to late adolescence. Nutr Health, 2007. 19(1-2): p. 143-61.
- McGinnis, W.R., Oxidative stress in autism. Altern Ther Health Med, 2004. 10(6): p. 22-36; quiz 37, 92.
- Duff J., Nutrition for ADHD and Autism, in Clinical Neurotherapy: Application of Techniques for Treatment, D. Cantor and J. Evans, Editors. 2013, Elsevier: New York. p. 357-381.
- Bourre, J.M., Effects of nutrients (in food) on the structure and function of the nervous system: update on dietary requirements for the brain. Part 1: micronutrients. J Nutr Health Aging, 2006. 10(5): p. 377-85.
- Sinclair, S.A. and U. Kramer, The zinc homeostasis network of land plants. Biochim Biophys Acta, 2012. 1823(9): p. 1553-67.
- Duff, J., Changes in brain electrical activity of boys with ADHD following neurotherapy, in Brain Sciences Institute 2010, Swinburne University: Melbourne. p. 482.
- American Psychiatric Association, A., Diagnostic and Statistical Manual of Mental Disorders. Fourth edition (DSM-IV). 1994, Washington: American Psychiatic Association